
Introduction and Healthcare Politics
One of the things I like about blogging is that it allows me to go into much more detail than a tweet or Facebook post. We unfortunately live in a world that wants to boil everything down to a short sound bite or tweet. “Crooked Hillary”, “Beat Cancer”, and “Medicare for all” come to mind.I consider myself to be politically independent, but living in Massachusetts does give me a pronounced lean to the left. As a cancer patient that owes my very life to medical treatment, you think it would be a slam dunk that I’d be all in on “socialized medicine” or “Medicare for all”, but something strange has happened.
As I began thinking and writing about my experiences and what I’ve learned, it occurred to me that our current system is doing a great job at improving the lives of cancer patients. I began to ponder the possibility of unintended consequences, and how complex this problem really is. It involves affordability of treatment (regardless of who is paying for it), which brings in income inequality. The cost of education and student debt is causing a shortage of doctors. Improving healthcare in this country will necessarily require addressing all these issues.
I’m feeling very verbose lately so this is intended to be the first of a multi-part series. Today I’d like to write about the scientific studies behind cancer treatments, how they are leading to dramatic improvements in outcome, but causing a cost problem that is increasingly referred to as “financial toxicity”. Many times now we are able to save the patient but bankrupt them in the process.
This verbosity may also mark a transition from simple blog posts to writings that resemble rough drafts of material that might end up in a book someday. My goals are to share the knowledge I’ve gained, provoke meaningful thoughts and discussions about cancer and health care, and also to entertain and generally be silly in the process. Laughter really is the best medicine.
Cavemen With Cancer
Let’s start by considering what used to happen to an advanced prostate cancer patient years ago, before medical treatments were invented. One day Gunga woke up and noticed his morning pee came out slower and had a reddish color to it. A short time later he started having back pain. His family commented that he was losing weight. He went on to die a slow and painful death over the next couple of months. Untreated prostate cancer is a nasty way to die.Gunga’s death was before the invention of suits and coffins, so funeral services were brief. They mostly consisted of getting Gunga’s smelly body out of the family cave. It was a simpler time. Geico was selling health insurance to cavemen at the time, which would have been 100% profit due to the lack of medical care, but it turns out cavemen hadn’t invented money and couldn’t afford their premiums. Geico pulled out of that market and continues to slander cavemen in their advertisements to this day.
Yes, this section borrowed heavily from “History of the World, Part 1” and Geico commercials.
Lupron and Testosterone
Fast forward to the 20th century. Healthcare is now a thing. A correlation between testosterone and prostate cancer has been found. If a man has prostate cancer and his testicles are surgically removed, the cancer stops growing. Hooray, he’s cured! Oh wait, no. It typically works for a few years, but the cancer soon returns. This is what’s called a “treatment failure”.Most men don’t like the idea of having their balls cut off, or to put it politely, opt not to have an orchiectomy. Instead, most men prefer to take a drug such as Lupron, which through chemical means stops the testes from producing testosterone. This is also referred to as chemical castration. Stop for a moment and consider that most men prefer to be castrated in order to fight cancer. It’s not clear how many of them say “I’d give my left nut to stop this disease for a while”, but the doctor probably replies “make it both and we have a deal”.
Castration, whether it be chemical or surgical, doesn’t get rid of all the testosterone in a man’s body. There’s a small amount that’s still produced by the adrenal glands. Treatment failure can happen by a number of means. Sometimes the cancer cells grow more testosterone receptors and that little bit of testosterone is enough to signal the cancer to continue growing. The more inventive cancer cells will actually figure out how to make their own testosterone, probably by turning on the same sequence of genes used by the testes. In any case, it’s all but inevitable that treatment will fail and the cancer will progress.
Let me introduce a couple terms that come up a lot in cancer studies. First, we have “failure free survival”. This is a measure of the time between when a particular treatment is started and when it fails and the cancer starts growing again. Death is also considered a treatment failure, even if the cause of death was being hit by a truck. Progression of the cancer can be determined by blood work or looking at scans. Scans are somewhat subjective so given the same scans you may get different opinions of whether the cancer is progressing depending on who you ask.
“Overall survival” is the time until the subject dies. Determining if a test subject is alive or dead can be done with a simple and inexpensive test. Better yet, there’s usually no disagreement between doctors over the interpretation of the test results. This makes overall survival the gold standard when measuring the effectiveness of cancer treatments. As noted above, it doesn’t matter if the cause of death was being sucked into a jet engine. Some studies will also measure “cancer specific survival”, which excludes non-cancer causes of death, but this can bring subjectivity back in and thus isn’t as good of a measure.
Note also that everything is about survival. Quality of life, which is definitely reduced without your family jewels, isn’t directly measured in these studies. It may indirectly be a factor, because some men won’t tolerate the side effects and will drop out of the study.
To summarize, imagine a man goes to his doctor and finds out he has advanced prostate cancer. Treatment with Lupron starts immediately. His symptoms lesson while scans and blood work show improvement. 30 months later his symptoms return with his cancer, and 6 months after that he passes away. His progression free survival was 30 months, and his overall survival was 36 months. Three years of Lupron costs roughly $50,000. Pricey, but somewhere between the cost of a sensible car and a college education.
Enter Zytiga
Meetings are held in a number of pharmaceutical companies. They talk about the poor survival of advanced prostate cancer patients. If only there was a way to deal with the testosterone that remains after castration. One company hits upon the idea of making a drug to block the testosterone receptor and names it Xtandi. Another company approaches the problem by interfering with an enzyme used in the production of testosterone and names it Zytiga. Executives at both companies see $$$ in their eyes thinking of the profits they can make if these drugs work out.Let’s focus on Zytiga, as that’s the drug I have direct experience with as a patient and has been the subject of several interesting studies. We’ll also ignore the process by which the idea of interfering with enzymes becomes a candidate pharmaceutical, because I have no clue how that happens. So starting with our candidate drug, how do we turn that into an FDA approved treatment? There are three phases of human studies to do that.
The first phase takes a small number of patients and gives them an increasing dosage of the drug. A quick word about drug dosages: “Effective dose” is the dose at which the drug has the desired effect. “Lethal dose” is the dose at which the patient dies. Drug safety is a function of the difference between these two doses. Phase one trials are more about finding a safe dose than finding an effective dose.
Phase two trials use more patients, typical in the hundreds, and establish that the drug is effective at the safe dosages determined by the phase 1 trial. With a prostate cancer drug, researchers would be looking for improving blood numbers and signs of tumor shrinkage in scans.
The third and final phase typically takes a thousand or more patients and compares the new drug to the existing standard of care. The intent is to determine that the new drug is somehow better than the drugs that have already been approved. These studies necessarily take years. After all, if many patients are living for three years on Lupron, you’ll need at least three years to show that your drug is better.
More terminology: most studies look at median overall survival. This is the amount of time until exactly half of the patients in a study group have died. It should not be confused with average survival. Average survival can only be computed after all participants have died. Median survival, by definition, can be determined when just under half the participants are still alive.
The phase three trial for Zytiga (https://clinicaltrials.gov/ct2/show/study/NCT00638690) went like this: Recruit 1195 men whose cancer was progressing after failure of existing treatments. 797 of them were given Zytiga with Prednisone. The other 398 were given a placebo with Prednisone. Then the researchers waited to see how long it took for 50% of the men in each group to die. The result: 450 days for Zytiga, 332 days for placebo.
That’s only about 4 months longer survival, which sounds underwhelming. Let me reiterate that this is a median survival increase of a large number of test subjects, and does not represent individual experiences. Some test subjects receiving Zytiga surely died very quickly as their cancers were aggressive and didn’t respond to treatment. But by the definition of median, about half the subjects in the control group were still alive a year later, while some in the Zytiga group had already died. A few subjects probably had a miraculous response to Zytiga, lived for many years, and were in a newspaper story about cancer patients who beat the odds. With 1,000 patients you’ll see all sorts of improbable things happen multiple times. The large number of patients is needed to get a statistically significant result.
This is the difference between a large scientific study and anecdotal evidence. When you are diagnosed with cancer, you hear every story about a friend of a friend who had terminal cancer, refused treatment, started eating broccoli and went into remission. I have no reason to doubt that such stories are true, but when you look at the experience of thousands of cancer patients, you find multiple stories of great results with modern medicine, and maybe one or two broccoli stories.
Okay, getting off my soapbox now. Based on the results of this study, Zytiga gained FDA approval and went on the market at a list price of around $10,000 for a month’s supply. It represented an incremental improvement in survival, but bigger and better things were about to happen.
STAMPEDE
The Medical Research Council in the UK has been conducting a huge prostate cancer study code named “STAMPEDE”. This is a huge study looking at the best time in the disease process to use currently available drugs and what combinations to use them in. One study arm is looking at “early Zytiga” in which it is prescribed soon after diagnosis instead of after other treatments have failed. (https://www.nejm.org/doi/full/10.1056/NEJMoa1702900)This study is still ongoing, but early results indicate a huge advantage for early use of Zytiga. Approaching the five year mark, half of the early Zytiga patients were still alive. This and other studies are showing that when used before Lupron fails, Zytiga improves median survival by around 18 months. Remember, that’s a median, so half of patients are doing even better than that.
Let’s look at some of the data that’s available from this study. If you read cancer studies, you’ll frequently see a graph called a survival curve that shows the percentage of patients still alive at various points in time.

This graph is the survival curve for the subset of patients with metastatic disease (the flavor of cancer I have). The blue line is for the “early Zytiga” group, the black line is where Zytiga is withheld until ADT stops working. That’s probably an oversimplification, but the point is that my understanding is that the primary difference between groups is WHEN Zytiga used, not WHETHER Zytiga is used.
Not long ago, patients diagnosed with metastatic prostate cancer had about a 28% chance of living for five years. The graph above stops six months short of five years, but that’s close enough to estimate five year survival. The black line looks to be heading to a 40% five year survival rate, which is better than 28% and is probably due to new drugs including Zytiga. The blue line looks to be heading towards well over 50%, possibly as high as 60%. In other words, about double the number of men live over five years.
While I’m diving into study data, here’s another graph. This one shows failure free survival. Remember failure free survival from a few pages ago? This is a graph of it.
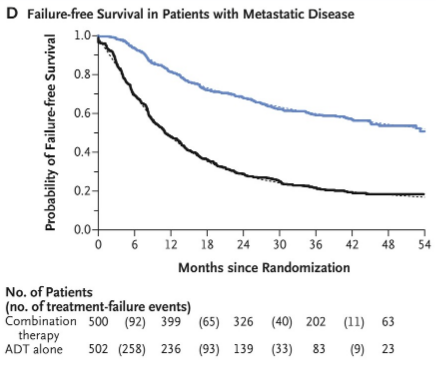
Let’s look at that black line first. This is the control group that only received Lupron (ADT). It tells you all you need to know about median times and how response to treatment varies greatly from individual to individual. According to this graph, the median time before Lupron fails is about 12 months. 12 months?!? What chance does anybody have to make it to 5 years? Actually, about a 20% chance. Look at how that black line flattens out on the right side.
This is how cancer treatment seems to go. You get some number of men that don’t have a great or lasting response to treatment, while others have a great response and live for a very long time. There’s not a lot of rhyme nor reason to who responds and who doesn’t.
The blue line is for the early Zytiga group, and after almost five years the treatment is still working for half the men.
Taken together, these two graphs paint a picture of a miraculous improvement in outcomes. Not only are men living years longer, but the number of men going well beyond the five year mark is exploding. This is remarkable progress in the fight against cancer. Except…
Financial Toxicity
Remember when I said that Zytiga cost about $10,000 a month? Did you notice how many men are living for 60 or more months while taking Zytiga the whole time? Yes, you too can beat cancer for five years for the low low price of $600,000. Oops, I forgot, you’re also on Lupron during that time as well, so that price is closer to $700,000. If you don’t have drug coverage and live in a nice neighborhood, you could sell your house for five years of living homeless.If you compare this to the earlier Lupron only example, you will quickly see that, approximately, survival has doubled while the lifetime cost of treatment has gone up by a factor of 10. I'm not too terribly concerned with the exact number, but did want to point out that these better treatments cost more per month and lead to longer survival, which causes the total costs to explode.
One caveat: Zytiga became available as generic Abiraterone in late 2018 for a much lower price of about $4,000 a month. This would make the 5-year total cost of Abiraterone and Lupron roughly $350,000. Yay, half price!
Remember Xtandi? That’s also roughly $10,000 a month, and no generic is available. Just to show I'm not making this stuff up:
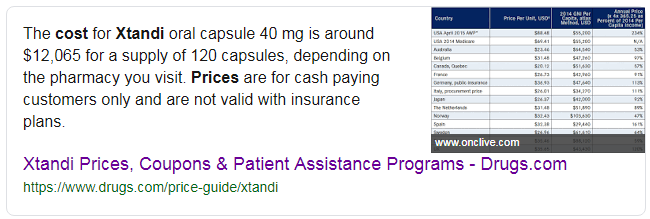
Another part of the Stampede trial is testing a combination of Zytiga and Xtandi. Let me paraphrase that study: Can we add a few more years to survival by doubling the monthly cost of treatment? If the answer is yes, treatment costs for the average patient will now run into the millions.
For now, I'm also going to ignore the issue of side effects accumulating as more medications are used in combination. Suffice to say some people view cancer treatment as paying a lot of money to feel like crap, "but at least I'm still alive".
These prices are a double edged sword. Pharmaceutical companies are rushing to develop newer and better cancer medicines due to the insane profits they can make. This is driving great progress in treating cancer, but for patients, insurance companies, and medicare, it effectively turns a medical disaster into a financial disaster. Arguing about private insurance versus medicare for all quickly becomes a debate about which one should go bankrupt. We need to control costs without removing the incentive for innovation.
But enough politics for now. I don't have any ready answer, just wanted to highlight the problem I see and say it can't be solved with a sound bite.
Coming up in Part 2: Bacteria, cancer cells, and why cancer can be so darn difficult to cure.


















